A summary of prevalence of non-communicable disease and cancer incidence in Wales - trends and 10-year projections
Rhys Powell, Publichealthwalesobservatory@wales.nhs.uk
Date published: 9 December 2024
Headlines
Using historic data, we have made projections for nine non-communicable diseases and cancer incidence up to 2033/34. We project that if nothing changes, such as the introduction of a health or policy intervention, all diseases and cancer incidence for both sexes will continue to increase.
We have studied historic prevalence data for a number of diseases, including diabetes, cardiovascular diseases, respiratory diseases and musculoskeletal diseases, as well as cancer incidence. This showed that this increase has been happening over the last 10 years, and in some cases longer.
Some of the change will be attributable to Wales’ ageing population. However, a number of risk factors, some of which are modifiable, also influence the likelihood of developing these diseases.
Count and percentage increase of adults with chronic diseases in 2023/24
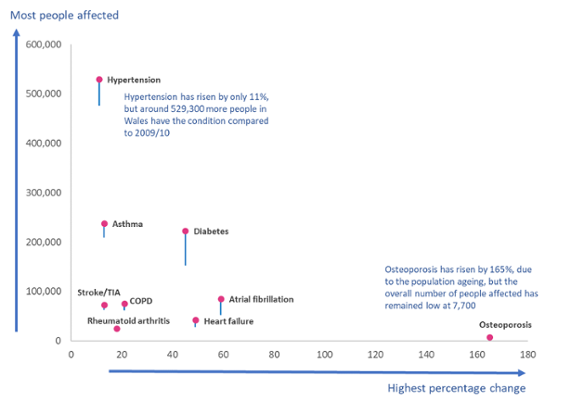
Figure 1: A chart showing a number of disease registers and the percentage and count change increase between when data was first recorded and the latest available data, 2023/24. The top of the lollipop shows the number of people with the condition in 2023/24. The bottom shows the number of people with the condition when data was first recorded. Quality and Outcomes Framework (2009/10 to 2018/19) and the Quality Assurance and Improvement Framework, Welsh Government)
Sections
- Overview
- Prevalence and incidence
- Projections
- Why is this important
- Data quality and interpretation
- Data files
Overview
The purpose of this article is to help policy, planning and decision makers understand the current prevalence and incidence of these conditions, and how it might look in the future if nothing changes, such as the introduction of a health or policy intervention, aimed at the factors influencing prevalence. This article is the first in a series of articles, that will focus on:
-
Prevalence, incidence and projections
-
Musculoskeletal disease
-
Cancer
-
Smoking
-
Mental health
We have already produced an article focusing on diabetes.
Prevalence and incidence
Prevalence is a measure that looks at how many known cases of a disease are in the population at any given point. Incidence looks just at newly diagnosed cases within a particular period. For diabetes, cardiovascular disease, respiratory disease and musculoskeletal disease we will be looking at prevalence, and for cancer, we will be looking at incidence.
There are two ways to look at prevalence and incidence, counts or rates. Counts show how many actual cases there are, and rates show the number of cases divided by the population at risk. Our analysis focuses on counts. We chose counts, as they are the most consistent data measure available to us over a long enough period to allow projections. Age-standardised prevalence rates adjust for differences in the age structure of the population between areas or over time allowing meaningful comparisons to be made. Some age-standardised analysis is available in our Primary Care Clusters dashboard and Cancer Reporting Tool.
As shown in table 1 and 2, over the years all these conditions have increased. Generally speaking, the more notable increases in prevalence tend to occur in middle and older age; however younger age groups are also affected. The forthcoming disease specific articles will look at the affected demographics in more detail.
Chronic condition register change from earliest available data to 2023/24
| Group | Condition | From | Count in 2023/24 | Percentage increase |
|---|---|---|---|---|
| Diabetes | Diabetes (aged 17+) | 2009/10 | 222,700 | 45% |
| Cardiovascular disease | Atrial fibrillation | 2009/10 | 84,900 | 59% |
| Heart failure | 2009/10 | 42,500 | 49% | |
| Hypertension | 2009/10 | 529,300 | 11% | |
| Stroke/TIA | 2009/10 | 72,400 | 13% | |
| Respiratory | Asthma | 2009/10 | 237,400 | 13% |
| COPD | 2009/10 | 75,600 | 21% | |
| Musculoskeletal | Osteoporosis | 2012/13 | 7,700 | 165% |
| Rheumatoid arthritis (aged 16+) | 2013/14 | 25,300 | 18% |
Table 1: A table showing a number of disease registers and the percentage and count change between when data was first collected and the latest available data. Percentages have been rounded to the nearest whole number and counts to the nearest hundred. Quality and Outcomes Framework (2009/10 to 2018/19) and the Quality Assurance and Improvement Framework, Welsh Government
Cancer incidence change from 2002 to 2019
| Group | Sex | Count in 2019 | Percentage increase |
|---|---|---|---|
| Cancer incidence | Men | 10,800 | 33% |
| Women | 9,600 | 21% |
Table 2: A table showing cancer incidence percentage and count change between 2002 and 2019. Percentages have been rounded to the nearest whole number and counts to the nearest hundred. Cancer registration data, Cancer reporting tool Welsh Cancer Intelligence and Surveillance Unit (WCISU)
Projections
Using the register and incidence data above, we have projected forward how they may look 10 years from April 2024. We do not expect these projections to be precise, and merely show a likely direction of travel should nothing change in between. For example, the introduction of a health or policy intervention aimed at reducing unhealthy behaviours, such as the introduction of smoking bans. More information on the method is available in the data quality and interpretation section, or you can contact us direct.
Projected change of chronic conditions from 2023/24 to 2033/34
| Group | Condition | Projected count in 2033/34 | Percentage increase |
|---|---|---|---|
| Diabetes | Diabetes (aged 17+) | 272,300 | 22% |
| Cardiovascular disease | Atrial fibrillation | 106,900 | 26% |
| Heart failure | 61,800 | 46% | |
| Hypertension | 565,900 | 7% | |
| Stroke/TIA | 78,400 | 8% | |
| Respiratory | Asthma | 256,400 | 8% |
| COPD | 84,800 | 12% | |
| Musculoskeletal | Rheumatoid arthritis (aged 16+) | 29,200 | 16% |
Table 3: A table showing a number of disease registers and the percentage and count change between the last observed data (2023/24) and projections in 2033/34. Percentages have been rounded to the nearest whole number and counts to the nearest hundred. Quality and Outcomes Framework (2009/10 to 2018/19) and the Quality Assurance and Improvement Framework, Welsh Government
Projected change of cancer incidence from 2019 to 2033
| Group | Sex | Projected count in 2033 | Percentage increase |
|---|---|---|---|
| Cancer incidence | Men | 12,700 | 18% |
| Women | 10,800 | 12% |
Table 4: A table showing cancer incidence percentage and count change between the observed data (2019) and projections in 2033. Percentages have been rounded to the nearest whole number and counts to the nearest hundred. Cancer registration data, Cancer reporting tool Welsh Cancer Intelligence and Surveillance Unit (WCISU)
As shown in tables 3 and 4, if current trends continue, and no additional action is taken to try to reduce the prevalence of these diseases, they will continue to increase over the next 10 years. Cancer incidence for both men and women is also projected to continue increasing.
Why is this important?
This analysis only looks at a select group of diseases; there are others that have not been analysed at this time. They all have one thing in common however, a direct effect on the health, wellbeing and quality of an individual’s life.
The day-to-day effects of these conditions can include, but are not limited to:
-
Regular monitoring of the condition through medical appointments, or at-home glucose monitoring for diabetes
-
Having to regularly take medication to manage a condition and reduce the risk of further progression and complications
-
Time required to attend medical appointments
-
Poorer overall health
-
Worse health outcomes should the individual fall ill
-
Greater chance of developing other diseases
-
Poorer quality of life, particularly with mobility and respiratory conditions
-
Effect on an individual’s ability to work.
Additionally, the management and treatment of these diseases has an impact on the NHS, including:
-
Cost to the NHS (prescribing medication, performing investigations, running consultations/clinics, cost of hospital admissions and providing treatments)
-
Resources required to organise and perform appointments and procedures, in terms of staff numbers and time required
-
Opportunity cost, meaning the diversion of resources from other patients
-
Wider economic and societal costs if individuals are unable to work.
There are a number of factors that can influence the likelihood of developing these diseases. Some are non-modifiable, such as age, sex and ethnicity. However, there are a number of modifiable risk factors and healthy behaviours, such as obesity, smoking and physical activity levels. There are also wider societal and environmental factors that play a role such as income, education, employment and housing.
These are commonly referred to as the wider determinants of health, as described by Dahlgren and Whitehead. This model describes how all aspects of life can influence an individual’s health, and can help us understand why people who are residing in areas associated with higher levels of deprivation often have poorer health outcomes. For example, from a financial aspect healthy food and membership to fitness facilities may be less affordable. They may also be time-poor due to the nature of their work, including having multiple jobs. This lack of time may mean they do not have time to prepare healthier meals or partake in exercise, including ones that may be relatively low cost.
Our risk factor article will look at some of these in more detail.
Data quality and interpretation
Prevalence data
The prevalence data are from the Quality and Outcomes Framework (2009/10 to 2018/19) and the Quality Assurance and Improvement Framework (2019/20 onwards) from Welsh Government. This data supplied by GPs shows the number of registered patients on a particular disease register and the total registered population.
Primary care registers should be interpreted with some caution, as some changes may not be due to an actual change in prevalence. As medicine progresses, methods may be developed to detect conditions more effectively, leading to better identification as opposed to an actual increase. Conversely, when QAIF replaced the QOF in 2019/20, the change in the contract regarding how data is collected from primary care has potentially led to changes in data quality, primarily a potential reduction in reporting, leading to an undercount of prevalence. This is particularly true when the changes are very small, as it is not possible to say with absolute certainty if it represents a true change or is due to a change in data collection.
The data comes from a single data source based on GP registered patients. As a result, it does not capture anyone who may be undiagnosed, or diagnosed but not registered. This means that the figures provided are potentially an undercount of the true prevalence.
Cancer incidence data
Historical cancer incidence data are from the Welsh Cancer Intelligence and Surveillance Unit.
Cancer incidence is available up until 2021, however 2019 has been used as the reference year. Due to the effect of COVID-19 on services, data from 2020 and 2021 is not well suited for projections or understanding long-term trends.
Projection methods
For our projections, we have used a standard time series model known as an ARIMA model. The model projects historic prevalence and incidence counts forward to 2033/34. We have also provided 95% upper and lower confidence intervals, estimating an interval in which a future prevalence might fall. These indicate that we believe with 95% certainty that the figure would fall somewhere between these counts, assuming current trends continue. These are available in the data download. The figure we refer to in the article, the central estimate, is the most likely estimate, given what has already been observed. The further forward we project, the less confidence we have in the estimates.
We do not expect these projections to be precise, and merely show a likely direction of travel should nothing change in between. For example, the introduction of a health or policy intervention aimed at reducing unhealthy behaviours, such as when smoking bans were introduced.
If you would like more information on the technical details of the projections, please do not hesitate to contact us.
Data files
We are aware that there can be issues downloading the data files in Microsoft Edge. If you would like the data, you may need to use a different browser, use 'Save as' if the data opens in an online tab or contact us at Publichealthwalesobservatory@wales.nhs.uk
Download the data in this article – Excel
Download the data in this article - CSV